In a few days I am heading to Hermosillo, Sonora to meet with the principals of a new palliative care residence, review some assisted living/long-term care homes, and join a colleague in San Carlos (two hours south near Guaymas) for a vital conversation on navigating the unexpected in Mexico.
We’ll be diving into the ‘why’ and ‘how’ of preparing for healthcare emergencies and end-of-life care in Mexico – a journey that requires understanding different laws, cultural nuances, and a healthcare system that can feel complex when you’re far from home.
My Death Educator and End-of-Life Doula colleague Marta Macbeth will share about her experiences with a dying loved one in San Carlos and Hermosillo as well as the use of cannabis for comfort care. Here is a photo of lovely Marta:
I will also share stories and focus on the importance of advance care documents plus building a support system if you are an expat. Together with Marta we will discuss the palliative care options currently available in the Guaymas-San Carlos-Hermosillo area.
Here below is a poster of the free, open to the public event if you have friends or colleagues in Sonora who may wish to attend.
Below the poster is a link to my blog, based on 11 years of hands-on experience, about Dying in Mexico and how to prepare.
Wendy Jane Carrel, MA, is a trusted older adult advocate and consultant who has hands-on experience with healthcare systems, senior care residences, and end-of-life care in Mexico, Ecuador, and other nations. She acts as a healthcare liaison providing informed, thoughtful guidance and curated, compatible care options for individuals, and for families and their loved ones. She is a speaker and published author on subjects related to senior well-being and a trauma-informed end-of-life doula. Wendy’s web site is http://www.WellnessShepherd.com.
While conducting research on health care and end-of-life options for older adults in Mexico, and volunteering at a Guadalajara palliative care hospital and “hospice” (not a term often used in Mexico, and not a term used by the hospital), I have witnessed both expected and unexpected deaths of Americans, Canadians, other foreigners, and Mexicans. In the case of Mexicans, the procedure following death is almost seamless, with rare exception.
Chapala Municipal Cemetery, Lake Chapala, Mexico
The question is, how will you prepare for such a situation if you are not Mexican?
Here is some of what I’ve learned in expat havens from Alamos to Ajijic, Mazatlan to Merida, and Tijuana to Oaxaca:
If you wish to save your family, other loved ones, and your neighbors considerable grief and time, it is important to understand what is involved when a foreigner dies in Mexico, and, to have a plan in place.
This goes for 18-year olds, 40-year olds, and especially for all persons over age 60.
Even though the subject is one many of us prefer to avoid, family and friends back home, as well as your local neighbors, will be grateful if you plan ahead. Planning ahead might even give you peace of mind!
WHAT TO BE AWARE OF
The system of law is different. If you are from Canada, England, or the U.S., you are accustomed to common law, not civil law based on Napoleonic code. The rules governing disposition of human remains in Mexico are not the same as at home. The time and bureaucratic requirements required to negotiate the Mexican system, post-death, can be daunting.
Laws governing end-of-life options and protocol are not federal. Laws vary from state to state regarding advance healthcare directives and the right to choose not to receive medical treatment if it is clear you are dying.
Mexico is a country with predominantly Catholic traditions. These traditions influence choices. If you are Catholic, the system may seem familiar, such as burial over cremation. If you had chosen to live in Buddhist or Hindu Asia, cremation would be a relatively easy matter involving fewer steps as cremation is common practice. Or, you could have opted for a Tibetan sky burial!
The Mexican culture, language, and way of thinking are unique. Most of all, procedures may be unfamiliar and complex.
PREPARING AHEAD FOR YOUR DEMISE & DISPOSITION OF REMAINS IN MEXICO
Legal Documents
The one key Mexican legal document you need to acquire for best outcomes is a “declaración jurada ” (more or less the equivalent of a living will) stating your dying wishes for comfort, how you wish to die, how you wish your body handled, your burial, cremation, and other desires. This document must be created before your demise. The declaración jurada will almost always insure your plan is followed. It is prepared by notaries (notarios), attorneys who are notarios, or attorneys who create the document and send you to a notario. The document is apostilled with the notario according to the Hague Convention which establishes a legal framework to resolve cross-border legal issues in family law and civil matters.
Current costs for the federal apostille are around 2200 MX pesos, 755 MX pesos for the legalization, 100 to 400 MX pesos per page for translation (many offices that assist foreigners write the documents in Spanish on one side, English on the other), about 30 pesos per page for official government certification, and between 1000 and 5000 Mexican pesos for the Poder Notorial (Power of Attorney) fee. Amounts may vary office to office. Refer to your local attorney or notary for exact amounts and details. Amounts may increase each year.
Note: Powers of Attorney (equally important for pre-death and health care complications), and wills regarding your property (usually a Testamento Publico Abierto) and fidelcomisos (for those owning property near the coastline or a border) are separate documents. Please consult with attorneys and notaries for specific advice. Once a year, older adults can receive a 50% discount in the month of September for wills relating to property (home, car, jewelry, and other assets).
Most notaries create and offer you two or three apostilled original copies of your declaración jurada. One copy stays with the notario. Carefully file your copies and if possible, create one photocopy for your glove compartment if you drive, place another in a binder or file at home, and scan and send a copy for cloud storage.
Note: Some funeral homes offer notarized Letters of Intention for cremation or burial. This, in addition to your declaración jurada, is a somewhat reliable back-up. These funeral homes will give you a card to carry on your person at all times; the card contains your name and other details plus their contact information. Not all funeral homes offer this service.
Your Advance Health Care Directive or Five Wishes from home is not valid in Mexico even if notarized, apostilled and translated into Spanish unless you get lucky.
You are best off incorporating preferences from your Advance Health Care Directive or Five Wishes (https://fivewishes.org/) into your Mexican legal document or declaración jurada. Several expats in Jalisco have chosen to do this with their attorney/notarios or attorneys and notarios.
As mentioned, many living wills/declaración juradas for foreigners, unless you live in a rural area, are written in Spanish on one half of the page, and English on the other. This is the most important document you can obtain relating to your end-of-life wishes.
Note: there is no guarantee your healthcare requests will be honored by doctors, hospitals, and ambulance services, just as in your home country. Your cremation request will be honored if it is in writing and your papers are presented.
Another helpful legal document exists if you are diagnosed with a terminal illness, the “voluntad anticipada” or “directriz”.
As of this writing, if you live in one of the Mexican states that have the Ley de VoluntadAnticipada (Advance Healthcare Directive law) you may refuse life-sustaining medical treatment. This document is created by a notario or your healthcare institution.
You may also incorporate your wish to refuse life-sustaining medical treatment in your living will/declaración jurada.
The states which have created and implemented the law of Voluntad Anticipada to date are Aguascalientes, Chiapas, Chihuahua, Coahuila, Colima, Guanajuato, Guerrero, Hidalgo, Jalisco, Michoacan, Nayarit, Mexico City, Mexico state, Oaxaca, Puebla, San Luis Potosi, Sonora, Tlaxcala, Veracruz, Yucatan, and Zacatecas.
Burial in Mexico
Burial in Mexico could be easier than shipping a casket home and less expensive, with one exception. Many cemeteries offer plots for purchase for a set period of time (usually six years) with the understanding that remains will be removed and buried elsewhere at the end of that period. Arrangements must be made in advance for relocation of remains or they may be removed to a communal grave.
There is now the option of green burial in the state of Guanajuato through the Elizabeth Kubler-Ross Foundation in San Miguel de Allende. At the time of this writing there is no other known green burial option in Mexico.
There are “natural” burials (linen shrouds, light wood caskets) in Jewish cemeteries at Lake Chapala, and in Mexico City, and Puerto Vallarta.
Note: There is less room at cemeteries in heavily populated areas. According to some city Pantheon (cemetery) directors, families with plots are burying loved ones 10 persons deep.
The population from Chapala to Jocotopec (north Lake Chapala) just south of Guadalajara, for example, is around 100,000, including 20,000 full-time ex-pats (numbers not exact). There are approximately 100+ deaths per year among the ex-pat community according to Chapala’s Registro Civil, Civil Registry office.
Ajijic Cemetery along Lake Chapala serves a population of 10,000-12,000. It is full unless a family sells you a plot there.
Ajijic Cemetery, Lake Chapala, Mexico
Cremation in Mexico
When death occurs in Mexico, local practices will govern how quickly a cremation can take place. In the state of Jalisco burial or cremation must be within 48 hours, or the body must be embalmed. There is one exception – a body can lie up to 30 days in refrigeration (if refrigeration is available and with permission) awaiting family members from out of country to view the remains. Then cremation or interment will take place. Cost for cremation in Jalisco, for example, is approximately 10,000 -15,000 Mexican pesos; costs for embalming, around 5,000 Mexican pesos. The prices escalate every year.
In Mexico your legal next-of-kin may request cremation or interment if you do not have a notarized living will with end-of-life wishes. It is unwise, however, to depend on good luck or miracles in this situation – again, best to have a Mexican living will, your declaración jurada.
Some churches in Mexico offer space for cremated remains in an urn or box in a mini-mausoleum setting. Here again, you are usually paying for a specified number of years.
Note: According to a U.S. Consulate web site, “if the deceased is to be transported between states in Mexico for cremation, the body must be embalmed. If the body is to be transported over 100 km a special transit permit is also required.”
Crematories
By law, a body is to be identified ahead of time. In Guadalajara, for example, no toe tags are used. Photos are taken of faces before the procedure. The name of the person is also written on a ticket. That ticket, serving as I.D., is inserted into a slot space outside the crematory machine.
Crematory Center, Guadalajara Municipal Cemetery, Mezquitan Country
Shipment of Remains Outside of Mexico
If you are American and wish your ashes or remains sent home, there is another step for a loved one or trusted advocate to complete after all Mexican death-related documents are obtained. (If you are Canadian, see the links in the Resources section below. Canadian procedures are not the same as American procedures). If your body has been cremated, a cremation certificate from the funeral home, an affidavit from the funeral director, and an original copy of the death certificate must be delivered to the nearest Embassy or Consulate. (See U.S. Government 7 FAM 258 DOCUMENTS TO ACCOMPANY REMAINS). If you die in a small city or rural area and cremation is your preference, understand the expense, effort, and permissions needed to fulfill this requirement.
According to the U.S. government, a consular officer will prepare a consular mortuary certificate to ensure “orderly shipment of remains and facilitate U.S. Customs clearance.” The certificate will be delivered to you in English and it will contain the essential information including cause of death.
As for shipment of remains in a casket, a U.S. consular officer will work to ensure that the Mexican funeral director and American funeral director are in communication to guarantee preparation of remains complies with local, U.S. Department of State, and federal requirements. All corpses going to the U.S. must be embalmed. The shipping time is approximately seven days.
Also note: DHL, Federal Express, and embassy diplomatic pouches cannot be used to ship cremated remains out of the country. There is no customs fee to ship remains to the U.S. Note: Shipment of embalmed remains in a casket outside of Mexico involves not only high cost, but red tape. Consider buying repatriation of remains insurance.
Other Details to Consider for Smoother Disposition of Remains in Mexico:
Someone to Act on Your Behalf, Preferably a Spanish-speaking Advocate
Are you a solo ager? Or a millenial digital nomad? Even if not, do you have at least three friends or neighbors in your community who will follow through with your wishes and instructions if you die in Mexico? Note: Do not depend on legal next-of-kin (spouse) or significant other to represent you. What if you both die in a car accident or other tragedy? It is best to delegate additional persons or a trusted attorney to take charge. Make certain this person understands and speaks good Spanish.
A Physician
Do you have a working relationship with a medical doctor who can be called immediately by the designated person or persons to declare cause of death and write the death certificate so an autopsy can be avoided? If you live in Jalisco do not call 911,an ambulance (Cruz Roja or Cruz Verde), the fire department (bomberos), or the police. Call the doctor, obtain the death certificate (Certificado de Defunción – delivered with three copies), then call the funeral home. The copies of the certificate are then delivered to the local Civil Registry (Registro Civil), the Ministry of Public Health, and INEGI (the National Statistics Office).
In places with several expatriates, funeral homes sometimes have doctors who can appear if your doctor is on vacation, but most doctors prefer a relationship with you before they will appear and sign a death certificate. Note: If foul play is suspected, an autopsy will be required and the police and fiscalia (the district attorney’s forensics department) will be involved.
Funeral company
Have you selected a funeral service or transporter to collect your body and handle your remains? Using a funeral service is necessary in most of Mexico, unless you are in a remote, rural village where you may be buried in a local cemetery.
Guadalajara Municipal Cemetery, Mezquitlan Country
Organ donation
Do you want your organs donated? Then your wishes must be written in your living will/declaración jurada or indicated on your Mexican driver’s license. Organ donations are handled by CETOT, the State Council of Organ Transplants.
Do you wish to donate your corpse for scientific study? If you die in Mexico City, your body may be welcome at UNAM’s Programa de Donacion de Cuerpo. Note: Many universities now use the TAQ Sistemas Medicos with synthetic human body parts for surgical instruction. The system comes complete with imaging equipment, computer interface, and surgical equipment.
Where to Place Remains. Do you wish your remains to stay in country or shipped home?
Chapala Municipal Cemetery, Lake Chapala, Mexico
Someone to Act on Your Behalf, Preferably a Spanish-speaking Advocate Part 2
Again, designate at least three people to oversee your affairs in Mexico in the immediate aftermath of your death. This is recommended based on witnessing situations in Ecuador and Mexico over a period of 15 years and accompanying distressed family members. Your ex-pat friends may travel quite a bit or may not be present at the time. Always plan for back-up. It is important understand and speak good Spanish.
Do your designees know which funeral service or transporter will collect your body? Do they know where your legal documents (passport, INM immigration green card, living will/declaración jurada – specific for cremation or burial, contact info) are and how to pay the funeral home if not pre-paid? Do they know where to locate your bankcard, cash, and/or documents 24/7? Do they have a set of your keys? Plan on leaving about 20,000 – 30,000 Mexican pesos or more for the certifying doctor, transportation, the funeral company, Civil Registry fees, and cremation so your friends are not left to raise funds.
Copies of Documents.
Your survivors will need several copies of critical documents – passport, residence card, living will/declaración jurada , death certificate, mortuary certificate, affidavit of Mexican funeral director, transit permit, et altri. The person(s) in charge must be told not to offer an original document to transit people, most bureaucrats, etc. – in most instances these entities receive copies. Place your documents in an easy to locate binder, scan them, and send them to cloud storage for retrieval. (You will have organized your passwords ahead of time and given them to your trusted designees).
Death Certificate (Acta de Defunción)
Who will obtain the Mexican government declaration of death with the appropriate stamps from the Civil Registry and the Ministry of Public Health? This is not only a death certificate but an authorization for burial or cremation. Some Mexican funeral homes have experience assisting with these matters, others not. Will your designees need to do it? Best to find out how to obtain the certificate in the state or province where you live so you can leave instructions. (See Resources section with links to information about death certificates in Mexico).
Register Death with Your Country’s Embassy or Consulate
Who will obtain the proper documents from the U.S. Embassy or Consulate, the Canadian Embassy or Consulate, or other foreign government representative in Mexico not only to register the death, but for remains transported home? Some funeral homes are accustomed to offering this service, others not. The embassy or consulate will prepare a Report of Death from the death certificate. Your family member or representative will use this document along with the Mexican documents if or when remains are transported out of Mexico. At the U.S. Consulate you are entitled to 10 to 20 original copies in English.
Spanish language skills are imperative
Depending on Spanish-speaking friends or Mexican friends during this process requires a Plan B. What if they are not available when needed? Have more than one person at the ready who can negotiate procedures in Spanish. There are a number of facilitators, translators, and attorneys who speak English or other languages, best to keep their information handy for your back-up group.
What happens if you die in Mexico, have no spouse, no next-of-kin, no legal documents stating your wishes, and no legal representatives?
Your body will probably be transported to a morgue, usually a SEMEFO (Servicio Médico Forense – Medical Forensic Service) building with refrigeration. Not all SEMEFO buildings have refrigeration or space, even if they have refrigeration. See video links at end of article with tours of SEMEFO in Guadalajara, Mexico City, Sinaloa and the Yucatan.
Your country’s representatives will be called. Each country has different procedures for handling such situations. Your body will probably be autopsied. Often, if no one claims your body, your remains will be placed in a communal grave in Mexico. Each state of Mexico and each rural area has different traditions and procedures.
Few people know where they will die or when. If you spend time in Mexico, or any Latin American country with deeply Catholic traditions, where family ties and support reign (i.e. you will be rescued and your loved ones will know what to do), as well as strict codes and preferences that may not be yours, please choose to prepare yourself.
Preparation hint: register your whereabouts and family contact information with your embassy or consulate The U.S. government, for example, has an excellent system for Americans at https://step.state.gov/. It is the Smart Traveler Enrollment Program and advises you of security risks in the place where you are living and assists with connecting family and others to you in case of emergency. Other places to register your emergency information are located in expat communities around the country. The registries are usually announced in local directories, magazines, English-language newspapers, or found by word-of-mouth. Some non-profit expat organizations provide registries as do churches and synagogues with English-speaking congregations.
End-of-Life Planning is critical for expats.
Create peace of mind for yourself, your loved ones, and your neighbors.
Note: Preparing medical directives for healthcare emergencies, and preparing wills, are subjects worthy of their own long articles and are not included above.
Note two: Physicians, hospital administrators, funeral directors, cemetery directors, city and province officials (including a district attorney forensics office), three attorneys, one notary, and a consulate were consulted with or interviewed in Mexico for this article.
Note three: If you are alone with no spouse, no children, and no one to rescue you, it is suggested you carry a copy of the funeral home card with contact information on you, plus a copy of key contacts including the notary public. When traveling, also carry a copy of your declaración jurada. If you have a car, it is recommended you keep a copy of your declaración jurada in the glove compartment.
Wendy Jane Carrel, MA, is a trusted older adult advocate and consultant who has hands-on experience with healthcare systems, senior care residences, and end-of-life care in Mexico, Ecuador, and other nations. She acts as a healthcare liaison providing informed, thoughtful guidance and curated, compatible care options for individuals, and for families and their loved ones. She is a speaker and published author on subjects related to senior well-being and a trauma-informed end-of-life doula. Wendy’s web site is http://www.WellnessShepherd.com.
You have permission to re-post the entire article or quote from the article when you include author’s name, biography, and contact information as above, and the copyright indicated below.
https://wdef.com/2018/09/19/morgue-director-fired-over-stench-of-157-corpses-in-truck/ September 2018 article reporting on two tractor trailers filled with unidentified corpses as there is not enough refrigerated space at the morgue in Guadalajara. A report by the English-language Guadalajara Reporter stated that corpses of two unrelated Americans, who died of natural causes, were stored in the tractor trailers, an indication that some stored corpses were identified first, not that it makes being stored in a tractor trailer palpable.
https://www.youtube.com/watch?v=kWNr53cWfxk Sinaloa SEMEFO, a report in Spanish about abandoned corpses and no refrigeration 2016, “muerte indigna.” Apparently a new building has been constructed since with refrigeration. Note: in places of extreme humidity and heat with no refrigeration, imagine the stench.
https://www.youtube.com/watch?v=5fNXN6XycPA According to the video, “drug dealer” tombs in Sinaloa represent the opposite kind of ending from an abandoned body left at the morgue. The Jardines de Humaya cemetery in Culiacán, Sinaloa, is known for its extravagant mausoleums, not all that dissimilar from the concept of the Mamluk tombs in Cairo Egypt’s City of the Dead (circa 642 AD). The video shows the tomb of Ignacio Coronel that apparently cost millions of pesos or dollars.
https://www.youtube.com/watch?v=B-mHof2axB4 According to this 2017 documentary video from Mexico City, if after three weeks no one identifies a body, it will usually end up in a communal grave. In another report, some bodies may go to a medical school for study.
https://tomzap.com/dying.html Dying in Puerto Escondido, Oaxaca, a 2013 report. At that time it was estimated one needed about 12,000 pesos to pay for cremation, now transportation and cremation will come to around 20,000 pesos, depending on the funeral home.
I am excited about Dementia Innovations, a group of fine folks in Wisconsin who have created LIVASU, a more affordable and hopefully sustainable option for memory care where couples and/or family members live with their loved ones. The project opens in July of this year. Here is a blog about the efforts based on my chat with their inspirational leader and Co-founder Mary Pitsch:
In an aging world where affordable memory care is becoming harder to find, LIVASU is pioneering a new approach in rural Wisconsin.
Inspired by the famous Dutch dementia village Hogeweyk, which opened in 2009 and serves 180 residents, this project brings a unique Midwestern touch to specialized senior living.
The name LIVASU—a portmanteau for “Living As Usual”—reflects the organization’s core philosophy.
“Our focus is a culture shift that restores autonomy to residents and prioritizes normalcy,” says Co-Founder and Board President Mary Pitsch of the non-profit Dementia Innovations, a social worker with over 30 years of experience serving older adults.
What is LIVASU?
Located on a 79-acre campus in the rural Town of Wilson, Wisconsin, LIVASU is a village of high-quality manufactured homes designed specifically for those with memory care needs. Unlike most institutional settings where residents pay a monthly fee or fee for life, LIVASU residents own their homes and live alongside their spouses, family caregivers, or on their own with support staff.
The model supports the Aging in Place preference of many Americans, especially boomers, the first of whom turn 80 in 2026.
LIVASU also provides a model that balances safety and freedom, empowering residents to choose what works for them emphasizes Pitsch.
LIVASU breaks away from “lockdown” restraints of traditional care by providing an open environment:
Natural Boundaries: The community is not gated. Instead of fences, the perimeter design uses “strategic landscaping to create natural barriers,” notes Pitsch, “it is typically Midwestern.”
Discreet Monitoring: Rather than physical restraints, the campus utilizes motion-sensor cameras that allow staff to monitor safety without infringing on privacy.
Psychological Comfort: By prioritizing quality of life over “safety at all costs,” LIVASU aims to eliminate the urge to “escape” or “elope.” When residents feel at home, the desire to leave the environment diminishes.
Site plan of LIVASU in Town of Wilson, Wisconsin:
Rendering of one section of LIVASU in Town of Wilson, Wisconsin:
What services and amenities are provided at LIVASU?
A gym, a spa, a grocery store, a farmer’s market, hobby spaces, village golf carts, on-site care and support staff, walking paths, and in Phase II a restaurant open to the public.
Who is LIVASU intended for and how did the concept develop?
“We came up with the LIVASU alternative care model for those who might not do well in traditional care settings,” shared Pitsch.
There are approximately 130,000 people in Wisconsin with Alzheimer’s.
The LIVASU concept, 10 years in development, began with a grass roots Task Force on solutions for dementia crisis situations for three years. That led to LIVASU’s formation and a 6-year journey researching traditional settings, noting what the challenges were and what was missing, what would work in the community, how to offer crisis prevention through environment, and just as important, how to make it affordable.
The Dementia Innovations team learned from emergency responders, the police, hospitals, and caregivers what could alleviate crisis situations.
On-line trainings were held remotely during COVID with Hogeweyk, and then a team travelled to The Netherlands for a site visit.
What does it cost to live at LIVASU?
Depending on the model, the 124 thoughtfully designed homes cost between $95,000 and $175,000. There is no property tax. “We feel owning your own home is key,” states Pitsch.
The homes are arranged with front porches facing other front porches.
There is a monthly service fee for care and support staff. The amount is determined according to needs. Unlike Hogeveyk, which is inside a gated campus, there is no nursing unit, though medicine at home and hospice will be welcome on the LIVASU grounds. Hogeveyk is for dementia residents only. Again, spouses and other family caregivers may live with their loved ones at LIVASU. Aside from possibly providing more stability for those with memory care issues, LIVASU could be a welcome solution for loved ones who prefer not to place their significant others in homes.
Solo agers with dementia may buy a home and pay for support services. Solo agers will need a fiduciary to handle financial and other affairs before and after their demise.
Once the village is full, priority will be given to Wisconsin residents.
The homes may be sold at any time by the current residents.
Note: The average U.S. price per month for memory care is $8,000/month not including doctor visits, meds, diapers, and transportation (double that at places on east and west coasts). Depending on the memory issue (Alzheimer’s – 70% of cases, Frontotemporal, Lewy Body, Vascular dementia, or other) lifespan from diagnosis can be from five to 20 years. When you do the yearly math the cost for care in a conventional setting is approximately $100,000 per year. In one of the video’s below you will hear the sobering statistics: 1 in 3 older adults die of dementia, and, by 2040 there may be a 53% increase in the number of persons who suffer from cognitive decline.
When will LIVASU open?
LIVASU opens in July of 2026.
“This has been a 10-year journey that started with a three year task force of community members. What we envision is all new, there is no road map, we are learning each day,” adds Pitsch.
There are other alternative and emerging non-institutional memory care projects around the U.S. located in San Diego, Baltimore, Kansas, and New Jersey. In 2003, Geriatrician Dr. Bill Thomas was one of the first to pioneer community-based care in residential settings for long-term care at his Green House Projects and Eden Alternative homes.
In the resource section below, you will find links to read about the Hogeweyk secured dementia village.
Wendy Jane Carrel is a trusted older adult advocate and consultant who has hands-on experience with healthcare systems, retirement options, senior living residences, and end-of-life care in Mexico, Ecuador, the U.S., and other countries. She provides informed, culturally sensitive transition guidance and curated options for families and elders. Her website is http://www.WellnessShepherd.com
We live in an aging universe, a universe where older adults live longer than ever before.
The need for housing and care, especially affordable housing and care, is growing in all three North American nations – Canada, Mexico, and the U.S. (See the Statistics section for expected growth by 2030 and 2050 at the base of this review).
In 2003, when working at a luxury senior residence in Rancho Mirage, CA, it was evident that healthcare affordability for U.S. older adults would become a challenge or become completely cost prohibitive, especially if dementia was part of the equation.
This revelation ignited my desire to explore international options.
I started investigating Ecuador, Mexico, and other destinations for medical care, long-term care, and end-of-life care, subjects that remain dear to me and those I serve.
My hands-on experience as a Mexico senior living consultant conducting due diligence over a period of 11 years in 18 Mexican states (there are 31. The Federal District of Mexico City makes 32) has kept me engaged and open to what’s happening on the senior living front. An excellent place for me to learn more was as a speaker and guest at this year’s CIAMAR Wellness and Senior Living Investment Summit 50+ to80, a conference produced by Javier Govi.
Govi is a “nearetiring” proselytizer and real estate entrepreneur who has believed in the growth of senior living in Mexico for American, Canadian, and Mexican retirees for more than a decade. His platform is focused on growth with corporate players from Canada, Mexico, Spain, the U.S., and other countries in Latin America.
My interest is in all sectors including smaller residences and intimate communities with sustainable futures.
Who attended CIAMAR 2025?
Between 150 to 200 persons attended the summit, gently modelled after NIC (National Investment Center) conferences in the U.S. with 1500 to 3,000 participants. The event was held at the Hotel Marquis Reforma in Mexico City.
Architects, bankers, real estate developers, senior living operators, tourism industry execs, one real estate appraiser, and entrepreneurs from around Mexico – Baja California Norte y Sur (Tijuana, Cabo San Lucas), Cancun, Cuernavaca, Leon, Merida, Mexico City, Puebla, Queretaro – and from other countries – Argentina, Colombia, Costa Rica, (Germany via Zoom), Panama, Spain, were present.
Below is a photo from the first day of the summit, almost an hour before we began.
What was on the agenda and who were the speakers addressing the opportunities?
Speakers from Latin America, mostly from Mexico, brought unique projects and perspectives, some are outlined further below.
These Latin American entrepreneurs see opportunity in attracting Americans, Canadians, and Europeans. One of the speakers referred to the current wave of this cohort as “el tsunami blanco”, the “white tsunami”. (An interesting comment as some expats in Mexico have Afro, Asian, and Latino heritage).
Latin American entrepreneurs are also focused on culturally compatible senior living for their own populations. Is there a way to meld the different cultures? This is a subject that remains open for discussion.
Some Mexican senior living homes thrive on hosting expats as their primary residents.
Despite the perception outside Mexico that Mexican elders are taken care of at home, many still are, there are senior living enclaves for Mexicans around the country, though far fewer than with Mexico’s neighbors north of the border. 31% of 11 million Mexican homes have at least one older adult (INEGI 2020).
According to INEGI (Mexico’s National Institute of Statistics and Geography, 2020) there are approximately 1200 senior living residences including assisted living/nursing care/memory care (often combined into one residence unlike American and Canadian systems). In 2017 there were an estimated 800.
The numbers for Mexico do not include independent living/active adult enclaves but do include corporate senior living, smaller private pay residences, non-profits often run by nurse nuns, and government homes. These numbers fluctuate as numerous small start-ups often close.
In Canada there are approximately 2,076 assisted living/supportive living/retirement residences according to Science Direct. Another source says Canada has 571 assisted living residences. (See Reference section below). In the U.S. there are approximately 32,000 assisted living communities with a total of over one million beds.
The “Bucket List” panel below with Javier Govi CIAMAR founder/producer, Wendy Jane Carrel, Kerri Moon, and Oliver Sahlmann
Three of us were invited to address the following question:
Who are the Americans, Canadians, and other foreigners considering Mexico for retirement and senior care?
We began our team presentation with a quick slide show of photos showing foreign residents in Mexico ages 60 to 100, couples and solo agers of diverse backgrounds (a growing number of Mexican Americans included), and those with diverse interests and preferences from no frills to resort-like settings.
Kerri Moon, an American entrepreneur who built one community at Lake Chapala and collaborated on the growth of the Namaste Community (another Lake Chapala expat community), pointed out, and we all agree, “the availability of caring workers who come from intergenerational households and are accustomed to respecting their elders could ensure superior staff-to-resident ratios giving Mexican senior housing a tremendous opportunity to succeed.”
Oliver Sahlmann, a business coach, former Volkswagen Mexico executive, and Mexico resident for 20+ years, shared about German retirees in Mexico. “They come mostly for the sun, and, in winter months.” He presented some charming cultural stories to give the audience a feeling for the German mindset.
The main points of my contribution were the diversity of ages, backgrounds, and interests, that no one plan fits all, and that most retirees from Canada and the U.S. prefer to Age in Place in communities with other expats. Fewer prefer living among locals but those who do often thrive.
The migration of Americans and Canadians to Mexico for retirement and senior care is not new, it has existed for decades. Numbers increased noticeably since 2008 (U.S. economic challenges), COVID, and as mentioned above – the realization that we are living longer and there may not be enough funds for retirement and healthcare. The U.S. does not have universal healthcare, Canada and Mexico do to varying degrees.
For older adults who have long-term care insurance and are independently wealthy healthcare is not an issue. But the reality is, even with U.S. Medicare, and continued rumors of cuts for Medicare and Medicare Advantage programs, some older adults are seeking alternatives and solutions in other U.S. states or other countries.
Here are some highlights from CIAMAR 2025 sharing pride of Mexico, sustainable projects, unique visions, plus mention of notable vendor/summit supporters:
Javier Govi invited attendees to invest in the future of senior living in Mexico and LatAm, invest in the concept of Near Retiring (bringing Americans and Canadians to Mexico), consider Pueblo Magicos for aging (see Reference section below for explanation of this government initiative for magical villages), and most of all offer dignity, quality of life, and exceptional healthcare. Govi is the author of Nearetiring: Baby Boomers, Snowbirds, and Summerbirds, a Great Opportunity for Mexico and Latin America in Spanish.
Mac Kroupensky – Mac is a thought leader who teaches corporations, companies, and government how to create innovative change and motivate people and teams. For 10 years he taught at IPADE, Mexico’s equivalent of the Harvard Business School or France’s INSEAD. “To be a great leader you must be a great human being,” is his motto.
Kroupensky has a super enthusiastic presence. He regaled the audience by asking them to imagine an ideal retirement place – a city of 150,000 with medical infrastructure, security, and new technology. He pointed to Sofia, Bulgaria’s thriving tech and arts scene, a city of old and new. Most of all, that perfect retirement place would offer the best of humanity, people who care. He then added, the Mexico/LatAm Senior Living Investment Summit would offer invaluable expertise and talent. He is right, it did.
In the photo below: Rafael Garcia Turban international developer, Oliver Sahlmann, Mac Kroupensky, Wendy Jane Carrel at CIAMAR Mexico and LatAm Senior LIving Investment Summit 2025
Antonio Gonzalez-Quiros F. , Director of Ballesol Mexico, was the keynote speaker. Ballesol is a Spanish corporation that for 40 years has developed 55+ resorts, residential apartments, and assisted living. Ballesol has assisted living facilities in Queretaro and Mexico City. Note: Spaniards and Latin Americans investing in senior living have much in common – culture, language, law, and a familiar way of doing business.
Ernesto Oechlar former banker, former CEO of a family-owned senior living residence, advocate for holistic senior living, organic food, and positive mind set. He is currently a consultant for Neuro Change Solutions (NCS), a global network of corporate consultants trained by Dr. Joe Dispenza teaching how to apply the neuroscience of change to increase employee engagement, collaboration, and productivity for business results. Delightful to converse with him and with Mac Kroupensky about differences of perception within cultures.
Marta Parra, Co-Founder and Co-Director of Virai Arquitectura, Spain. She was one of the last speakers and I wish more attendees could have listened to her enlightened presentation about creating accessible spaces and person-centered memory care with the energy of light, located in nature, and more. She is a pioneer in neuroarchitecture and sustainability for hospitals and senior living residences in Spain, Africa, and Latin America. Her slides and presentation were excellent. For more information see https://www.virai.eu/
Architect Carlos Sanchez of www.gomezplatero.com was a pleasure to listen to and learn from. He studied architecture in Torino, Italy and has worked on senior living projects in Medellín, Colombia and in Uruguay.
Mario López is the founderof Taxáre. He is a real estate appraiser, consultant and enthusiastic investment project manager for real estate businesses. You can find him as “Mario El Valuador” on Instagram, Tik Tok and his podcast Un Express de Real Estate on You Tube @soymariolopez. He showed us drawings of an eye-catching urban city design for Tijuana intended for retirees and others – modern towers, gated, secure, flat and walkable, alongside the Pacific Ocean, with sustainable architecture, lots of gardens and amenities. If and when such a project is manifested, I can see folks with this concept as their aging in place vision filling it up fast. Based on my several due diligence visits to Tijuana, the city would benefit from a project such as this.
Juan Pablo Payró an Architect/Masterplanner/Designer/Developer shared about Agrihoods and Wellness Community projects in Queretaro, San Miguel de Allende, Holbox, Bacalar, and Los Cabos. He is a co-developer with Javier Govi’s Grupo AMAR. I contacted him to share photos or a website but have yet to receive a reply.
Salvador Rivas, an articulate, cultivated British-Mexican architect, has worked on prestigious international projects. His web site is www.srivasarchitects.com . I contacted him for information related to senior living projects but have yet to receive a reply.
There were many worthy presenters. Apologies to those not mentioned.
A special shout out to Jose Manuel Diez for his elegant, gracious energy as Master of Ceremonies and to the amazing AMAR and CIAMAR support team who produced this event.
Attendees I also appreciated meeting:
Juan Jose Perez Rifel shared with me an appealing project for Queretaro, one of my favorite Mexican cities. He is with www.st-austin.mx (see concept photos at the website). As I understand St. Austin owns the land. The first project is an eco-sustainable hospital which will serve as the property anchor with plans to expand to a medical district with doctor’s offices, a senior living residence (no precise details), a commercial center, gardens, and more. I am eager to see it when it is built.
Visiting from Lake Chapala was Jorge Garcia de Leon who is head of operations at Rancho Salud Village, see www.rancholasaludvillage.com or their Facebook page. His father-in-law owns the land in this eco-friendly, holistic, sustainable, multicultural, co-housing community of homes for Aging in Place. I have witnessed the growth over 11 years from two homes to a plan for 21 and eventually 30+ with pool, vegetable and herb gardens, and more. I am a fan of Jaime Navarro, his lady Sara, and their passion for healthy, independent living.
Roberto Madruga Avensa of Mexico City has “four legally clear parcels for development” for an Aging in Place/Wellness project in the Pueblo Magico (magical village) of Ixtapan de la Sal. The project is known as Reserva Reforma and there is no website yet. Sr Madruga envisions a completely flat, walkable community with local healthcare within five minutes, a hospital you would be flown to by air ambulance if needed, living spaces with doors, floors, and more following the 150 Residencial Universal Living Design standards. Sr. Madruga’s wife is a geriatrician. They have travelled to Italy, Spain, and Switzerland to look at senior care. The Reserva Reforma concept would appeal to American and Canadian couples and solo agers if and when such a project is built may be a few years from now. In any event, the vision is a match with many folks who wish to move to Mexico, Baby Boomers especially.
Alejandro del Rio of Leon, Mexico. Family property on many acres in nature with a villa, a large home, lots of green trees, brick walls. It has been or is being converted into a senior living residence. See https://www.plenityland.com/ for photos and contact information.
Nelly Vasquez Sanchez of Gravasa Immobiliaria in Puebla and Oaxaca is a real estate agent and a newbie to the senior living world. She shared with me she attended the conference because she wishes to learn how to provide for expat residents. She paid attention to each presentation. She was a joy to get to know as she represents a younger generation that has an interest in aging. https://www.facebook.com/igruvasa/?locale=en_GB
Mauricio de la Cerda, VP Growth for www.angela.care was at a vendor table sharing how to receive pills in a pill pack organized by day and time (breakfast, lunch, dinner), delivered to you at home. Angela Care works in collaboration with Amazon Pharmacy.
Vendor Roberto Sanchez of Gerflor.com, a French flooring company, shared my kind of waterproof, antimicrobial, soft to fall on, quiet, no glue, fast installation flooring. I wish this flooring was mandatory in Mexican residences as injuries from falls could be less severe. Most residences have slippery tile flooring. I also had a secret desire that the Marquis Reforma Hotel where the summit was held would remove its marble floors. We were there in rainy season!! Here is the GerflorUSA website: https://www.gerflorusa.com/
Where is the money?
With the talent I witnessed and all the possibilities shown on multimedia around the conference center (some visually inviting, stunning in fact), I was mystified. I wondered why so many worthy older adult projects presented at the summit have not been built.
What has prevented architects, developers and others from manifesting their visions?
If I had not been breathless and a bit under the weather, nor missed the presentation that may have explained more “Where is the Money?” I may have learned more. Kudos to CIAMAR for the discussion.
So, I canvassed Mexican speakers and attendees and asked if they would please share what they see as obstacles.
The answers included government bureaucracy (heard this several times, heard this the most), challenging local laws requiring 2-3 years for permission to build, issues with land permits, financing, construction, and “voluntad” or will power and motivation for investment in this sector.
There is a growing venture capital market in Mexico of local and international investors. Most of the capital is being invested in technology, especially fintech.
Many architects and developers in senior living are essentially like movie producers. They create an idea, develop it, and shop it from place to place for financing.
It requires remarkable resilience and will power to be a Mexican entrepreneur in the senior living sector.
CIAMAR 2026 will focus on technology in senior living.
Summary
The need for senior living – housing and care, especially affordable housing and care, is growing in all three North American nations – Canada, Mexico, and the U.S.
For several decades Mexico has been a destination for Americans and Canadians. Now, with dwindling retirement funds, healthcare plans that are not flexible, and overall rising costs for housing and healthcare, the opportunity for more development is evident.
Senior living south of the U.S. border may be a continuing retirement trend.
Growth is slow as developments are often stalled by government bureaucracy, land permit issues, the ability to raise capital, and more.
Some Mexican developers are focusing on generations age 50+, especially those who are active and fit, seeking affordable luxury and a wellness environment.
Wendy Jane Carrel is a trusted older adult advocate and consultant who has hands-on experience with healthcare systems, retirement options, senior living residences, and wellness programs in Mexico, Ecuador, and other countries. She provides informed, culturally sensitive transition guidance and curated options for families and elders moving to Latin America. Her website is http://www.WellnessShepherd.com
Statistics for burgeoning population growth in North America:
Canada – 7.6 million older adults representing 18.9% of the population according to Statistics Canada 2024. Statistics project seniors could make up 23% of the population by 2030 and nearly 26% by 2068
Mexico – 10.6 million adults over age 65 according to INEGI the Mexican Statistics Bureau, and Statistica.com. AARP International suggests older Mexican adults will represent 30% of the population by 2050 an increase of 277%.
USA – The number of Americans 65 and older is projected to increase from 58 million in 2022 to 82 million by 2050 (a 42% increase) according to a 2024 study by the Population Resources Bureau.
I am on my way to Mexico City to speak at a Senior Living Summit being held at the Hotel Marquis Reforma September 3-4, 2025 about the growing need to create evolved, affordable, holistic enclaves of well-being for older adults to age in place, age in community, and more, a subject on my mind since 2003.
Quick history:
In 2003, when serving as nighttime administrator and day time admissions and marketing officer at an exemplary (still is) memory care campus in Rancho Mirage, California, (thank you owner and mentor Floyd), the writing was on the wall.
Unless you are blessed with excellent health your entire life and have experienced no accidents, in the U.S. the cost of adequate long-term care at home or in a residence, could easily require up to $1 million per person with 2025 fees and pricing. With long-term care insurance at several hundred dollars a month, only 80% of costs would be covered.
This awakening was the impetus to look internationally for more affordable options with quality care and medical infrastructure. Mexico and Ecuador, by virtue of proximity, were places I conducted due diligence and developed hands-on experience with locals and expats, as well as other nations farther away.
Thankfully, as a trusted older adult advocate and consultant I have met like-minded souls on my path including Mexico’s Javier Govi, the « nearretiring » proselytizer and real estate entrepreneur behind CIAMAR’s 9th edition Wellness and Senior Living Summit for 50+ to 80.
About 100 to 150 persons are expected to attend the gathering gently modelled after NIC (National Investment Center conferences in the U.S. with 1500 to 3,000 participants).
The concept to develop and expand senior living options is growing in Latin America as the silver tsunami is not just an American/Canadian/European phenomenon, it is worldwide.
Attendees will be real estate developers, venture capitalists, architects, brokers, folks from the tourism industry, and senior living operators who will meet, greet, and assess future potential for collaboration.
I will be on the Bucket List panel with two others to talk about expats who migrate to Mexico and other countries in Latin America and what their expectations are.
If you are unable to access it, here is how my bio reads:
Wendy Jane Carrel
Founder, Wellness Shepherd
A trusted older adult advocate and consultant who has hands-on experience with healthcare systems, retirement options, senior living residences, and end-of-life options in Mexico, Ecuador, and other countries. She provides informed and thoughtful transition guidance and curated options for families and elders moving to Latin America.
Looking forward to this adventure!
I hope to report about the experience and my findings after the summit.
Nestled in Mexico’s highlands, Aguascalientes charms visitors with colonial architecture, clean streets, wide sidewalks, shade trees, and a warm community spirit. About 1.5 million residents live at 6,194 feet above sea level, an easy drive on the highway from Jalisco (three hours from Guadalajara). Known for its safety and relative tranquility, Aguascalientes surprised this newcomer. During my three-day stay persistent winds became an unexpected part of the city’s personality.
Founded in 1575 by royal decree of King Phillip II of Spain, the city’s original name was Villa de Nuestra Señora de la Asunción de las Aguas Calientes (Village of Our Lady of the Assumption of the Hot Waters). Citizens are amusingly referred to as hidrocalidos or hydrothermal people.
Mini-park in central Aguascalientes:
Immaculate street with residences and shops in central Aguascalientes:
Aguascalientes is an industrial city. Major companies present are GM, Honda, Mazda and Nissan. Other notable companies manufacture medical equipment, electronics, car parts, and textiles. Years ago, Aguascalientes built trains. The original station still stands as a museum and there are restored train cars to see.
Not surprisingly, among the expat population estimated around 1,000, there are several Japanese. Trip Advisor lists 34 Japanese restaurants (not all Japanese owned).
A glimpse of what I experienced related to older adult activities, care, hospitals, and end of life:
Older Adult Socialization in Community
Club de la Tercera Edad is a public center for older adults run by CONACYT, the national counsel studying science and technology. When I arrived, there was a danzon class. Danzon is a Cuban music and slow dance tradition, immensely popular in Mexico and other parts of Latin America.
DIF and INAPAM Older Adult Activity Centers Both DIF (Desarrollo Integral de la Familia) and INAPAM (Instituto Nacional de las Personas Adultas Mayores) are government run centers offering activities. They are separate entities but sometimes collaborate. DIF addresses entire family needs and is more about social protection of vulnerable populations. It offers adult daycare centers, psychosocial support, food programs, medical attention, recreational activities, and more. INAPAM is focused on older adult legal rights, transportation discounts, medical and cultural services.
On another trip I hope to meet Aguascalientes DIF director Aurora Jimenez Esquivel, known for her innovative initiatives including a popular travel program to visit nearby states known as “Gigantes Viajeros”. If you have access to Facebook, there are charming photos with older adults from Aguascalientes enjoying a trip at the FB page of Aurora Jimenez Esquivel. The link would not post when I loaded it here.
Señor Sebastian As I made my way to the Panteón de los Ángeles y La Cruz, thirst led me to a sunlit corner store not far from the cemetery gates. There I met the venerable octogenarian you see in the photo whose warmth seemed to animate the whole neighborhood. With his son by his side, he presides over the store like a sage, sharing stories about local elders and aging in place. He graciously pointed me to the entrance of the cemetery. After wandering the peaceful grounds among small and large gravestones, I returned to thank him —feeling, in that moment, not just like a visitor, but welcomed to Aguascalientes. Memorable encounter.
According to INEGI (the Mexican government statistics bureau) and Google, there are about 14 long-term care residences. (In Mexico long-term care is, with some exceptions, all in one – assisted living/memory care/nursing).
I focused on homes in the city center and visited seven to get a feeling for environment, providers, residents, and care.
Three assisted living/memory care homes had closed, one during COVID. Most places were basic, clean, modest, and dark, yet each with devoted caregivers. Residents in some homes seemed thrilled to have a visitor.
I was warmly welcomed at clean, efficient, light-filled Residencia de la Roble which houses 33 older adults including Mexican-Americans who prefer to age in their native Aguascalientes. Care costs are about $700/month USD (13,000 pesos/month) for shared rooms (there were two single rooms). Included in the fee: nutrition with customized diets, television and activities, laundry, medical care by the owner, a geriatrician, and most of all what appeared to be loving, energetic care by devoted nursing assistants. Note: Many Mexicans are accustomed to sharing space. The concept of privacy and your own room is often found with families who are well-off.
Here are photos showing a shared room with pristine, well-organized clothing and linen storage:
There is no website for Residencia de la Roble but you may find several photos of its high energy, activities, and sweet residents and caregivers on Facebook at Residencia para adulto mayor “El Roble”. https://www.facebook.com/profile.php?id=100064126566555
On my next visit I wish to tour Estancia Geriatrica Villas Juan Pablo as I had originally planned. It is a privileged residence in a park-like setting, also with lots of light, a few miles north of the city center. You will find photos at https://estanciageriatricavjp.com/ The environment reminds me of countryside care homes outside Quito, Ecuador – wood cabinetry, vistas of green meadows, tranquility. Under “instalaciones” there are photos of private rooms. The monthly prices at Villas Juan Pablo would be double, or more than double, the costs at Residencia de la Roble.
Note: prices for long-term care in the state of Aguascalientes are less than in the state of Jalisco (home to Guadalajara, Lake Chapala, and Puerto Vallarta). The Aguascalientes homes cater to local Mexican families.
Hospitalsand Dental Care
Aguascalientes has an impressive medical infrastructure with hospitals both public and private. Hospital MAC (there are two, one in the north the other in city center), Centro Hospitalario de Aguascalientes, Star Medica, Centro Medico la Salud, Hospital Cardiologica de Aguascalientes, Medica San Juan de Aguascalientes, Hospital Fundación Medica México Franco Brasileña plus a plethora of other options for specialized medical care as well as dentistry.
Emergency Care at Hospital MAC
The third night of my visit I awakened around 10-10:30 p.m. feeling tingling down my right side and leg. My first thought, oh no, not a TIA/stroke!! But I was able to speak. The sweet elderly man on night duty at the hotel suggested a taxi to the Red Cross. I wished for a hospital. I was super weak and dizzy yet decided to slowly walk to a nearby hotel. The night duty clerk there suggested Hospital MAC, a few blocks away.
There are about 30 MAC hospitals in the country. I had visited others and felt confident. I was especially encouraged because I could see the hospital tower from the front door of the hotel. I walked slowly but surely about four short blocks and made it to the emergency room. A nurse promptly greeted me, took my name, invited me to a room, took my vitals. I was then escorted to meet Dra Nancy originally from Mexico City and a graduate of UNAM. She was amazing – attentive, kind, professional. A thorough assessment of eyes, strength in arms and legs, heart, walking etc. Thankfully I was going to be okay. I was dehydrated (first time ever and quite a lesson) and had a bit of heat stroke from walking in the sun from early morning to sundown. The hospital experience was a gift, and I remain grateful to all who assisted and cared for me at the hotel as well.
Palliative Care and End-of-Life Care
Pain relief for life-limiting illness is offered by 14 anesthesiologists with palliative care credentials at hospitals and clinics. Two of the physicians drive from Guadalajara. According to a list of medical providers, there are 20 geriatricians. In-home pain relief for end-of-life is offered by at least two geriatricians.
All assisted living/nursing homes attend to end-of-life.
One residence, Hogar del Abuelo Maty, was founded with supportive end-of-life care in mind. It is in the countryside one hour to the northeast of Aguascalientes.
The home, opened in 1981, is named in remembrance of Matilde (Maty) Dubroy de Villanueva who was accompanied at end of life by her daughter Carolina Villanueva de Garcia. The profound experience inspired Señora Carolina to build the hogar where every elder could have a dignified death with compassionate, personalized care.
The current administrator of the non-profit is the founder’s son, Carlos Garcia Villanueva. Care is provided by nurse nuns of St. Vincent de Paul. The nuns have a long and rich history of companioning the infirm and those at end-of-life. The website with photos and videos reveals more: https://www.hogardelabuelomaty.org/
While I did not encounter any modern-day end-of-life doulas in Aguascalientes, Mexico, non-medical, psychosocial spiritual support has been a community tradition for centuries. Local women known as “parteras” assist not only with birth but have a significant role supporting families and individuals during the dying process.
Funeral Home Arriaga
Toward the end of each day, I passed Funeraria Arriaga on the way to my hotel. Families waited inside where there are four viewing rooms and a place to sit and sip coffee or tea. Or, they waited in front of the building. There is a florist across the street.
Most Mexicans choose burial in a coffin. For those who choose cremation, the cost with this funeral home is between 9,000 and 20,000 pesos ($470 to $1000 USD) depending on whether there is a memorial service. According to Funeraria Arriaga there is no refrigeration in Aguascalientes but there is embalming. (Refrigeration is possible in Jalisco to create time for family members arriving from far away to view the deceased). The Boinita Group advertises green spaces for cremains (ashes) in Aguascalientes as well as Cancun, Hermosillo, Merida, and San Luis Potosi. https://boinita.com/en/green-niches-of-funerary-forests-in-mexico/
National Museum of Death
The museum, which opened in 2007, exhibits death-related artifacts from pre-Hispanic times to the present from the personal collection of Octavio Bajonero Gil. The 2,000 or so items include sacred religious paintings, sculptures, objects d’arte, and more. They are displayed in three connected buildings of a restored 17th century convent that once housed Franciscan monks. The property is now owned by the University of Aguascalientes.
My experience was not of the macabre. Some items show the unique Mexican sense of humor.
At the entrance of the museum is a gift shop where you pay an entrance fee of 20 pesos ($1 USD). It takes 45 minutes to an hour for a self-guided tour. If you are lucky you will have university student Antonio accompany you to the basement to see reconstructed gravesite remains. The photo below was taken in the basement:
Later, multi-lingual Jesus from Mexico City who delighted me with his Italian might lead you through the floors and buildings.
The museum produces 200 or so events per year including the October/November Day of the Dead Celebrations. At the writing of this post the calendar of events for the 2025 Annual Festival de Calaveras (skeletons) has yet to be posted.
Museo Posada This museum is dedicated to the collected works of Aguascalientes native Jose Guadalupe Posada (2 February 1852 – 20 January 1913), a political satirist/caricaturist, engraver, and printmaker known throughout Mexico as the father of La Calavera Garbancera/La Catrina, a female skeleton dressed to the nines that is seen each year at Dia de los Muertos/Day of the Dead ceremonies. During the presidencies of Portfirio Diaz (1876-1911) Posada introduced skulls and bones as political and cultural critique. La Catrina indicates death comes to all, including politicians and the super wealthy. Here below is a Catrina from the Museum of Death:
Wendy Jane Carrel, MA, is a trusted older adult advocate and consultant who has many years of hands-on experience with healthcare systems, retirement options, senior living and wellness programs in Mexico, Ecuador, Italy, the U.S., and beyond. She provides culturally sensitive transition guidance and curated options for families and elders domestically and internationally. Wendy’s web site is https://www.WellnessShepherd.com
In Mexico I have enjoyed exploring Pueblos Magicos (magical towns) from Alamos (Sonora in the north) to Izamal (Yucatan in the south), learning about Aging in Place/Aging in Community (which most Mexicans do), healthcare, and end of this life traditions.
Magical towns are designated by the Mexican government SECTUR (Mexican Tourism Board) as part of “Mexico desconocido” or unknown Mexico – towns or villages representing the cultural diversity of the country.
Below is a photo along the malecon adjacent to Rio Calvillo (the river) near the entrance to Calvillo a pueblo magico in the state of Aguascalientes.
I recently had the pleasure of visiting Calvillo, Mexico’s leading producer of guavas. There is far more to meet the eye than guavas, and, there was that feeling of magic.
What immediately struck me on arrival at the bus station was how clean the streets are (no trash, no stains), how flat the city is (mostly), how safe and flat the sidewalks are, how immediately friendly the people were, and how unpolluted the air seemed. It was a breezy, sunny weekday.
Just a few minutes away, down Calle Jesus Gomez Portugal to the left of the hallway exit, I stopped outside a space flooded with light and inviting aromas. A local restaurant, Gorditas Jenny. Smiling ladies beckoned me to enter for a look see. Fresh, unadulterated breakfast food in an immaculate setting served from 8:30 a.m. to 1 p.m. Yes, I tried it and wish to return! Thank you, ladies!!
Again, a warm and welcoming reception on arrival. The center offers painting (part of a program called “pintemos la magia de Calvillo” – let’s paint the magic of Calvillo), tai chi, chair exercises, handicrafts, carpentry, meals, trips, and resources for aging. In the following short you will hear precious elder Salomé Salas, a 94-year-old, joyfully share in Spanish why he loves the center, and you’ll get a glimpse of some of the activities. https://www.facebook.com/reel/3714970688791551
Asilo San José (originally Asilo de Los Ancianos Señor San José) is the only assisted living/nursing home in Calvillo. It was founded by the Catholic church and a group of locals and continues to be supported by the church, the locals, and a group of Mexican/Mexican-Americans from Santa Paula, Ventura County, CA, “citrus capital of the world.” As with many Mexicans who emigrate to the U.S., folks from Calvillo and surroundings send funds or return home to support the local community. Those who were born here often prefer to return to die or be buried.
Front of the Asilo San Jose Assisted Living/Nursing Home in Calvillo below.
Over 50 residents, men and women, reside on the spacious campus with three sections of housing. Most rooms are shared, two to a room. When I arrived, elders in wheelchairs were accompanied from mass at the chapel back to their rooms or recreation hall. I met with lovely assistant administrator Maria who graciously showed me the living quarters, the perfectly organized laundry and wardrobe area, the dining area, the meds room, and the offices. We agreed I would not take any photos. I was grateful to feel a sense of attention and care from her and the support staff as they looked after their charges. Without spending more time, or talking to community members, it is difficult to assess more. What was clear, however, is that the residence was welcoming and the residents clean, smiling, and mostly disabled, one severely disabled/bed-confined with an attendant. Each required round-the-clock care perhaps not possible in their homes. Below is a link to a video filmed 10 years ago which offers an idea of the environment, now re-painted and more lively.
There are three small hospitals in town: Hospital General de Calvillo, IMSS Unidad de Medicina Familiar, and the Clinca del Valle. I was unable to manage site visits, but I understood from locals that for more serious medical challenges some folks go to Aguascalientes an hour away by car or bus. I noticed medical and dental offices in the city center.
Parrochia del Señor del Salitre
The beautiful baroque parish church has three magnificent domes adorned with frescoes. It is dedicated to the patron saint of the city, Lord of the Saltpeter. According to city legend a group of older adults saw a miraculous appearance of the Lord on the parish spot before the church was built around 200 years ago. The colors inside are gold, light pink, and light blue.
The people of Calvillo appear to be deeply religious.
It was a remarkable synchronicity that I arrived at the church in time to attend mass for a beloved older woman. The church was full. I stood in the back. Mariachis waited at the exit. After the mass they accompanied the woman’s casket to a waiting car.
The woman’s family sat in the van behind the white hearse. Music played for blocks around the church and down Avenida Revolucion to the Cemeterio Señor del Salitre about a mile away.
The gentle words of the priest at mass, the reverence and grief of the attendees, the mariachis, and the atmosphere were deeply moving. I was simply a bystander. My eyes and heart welled up with tears off and on. A blessed experience. I am thankful to the fellows from Funeraria Carrillo who shared some of the details.
National Museum of Magical Towns It was a nice surprise to walk down Avenida Benito Juarez in the afternoon and discover this beautiful museum which I did not know existed until I walked by!!
The photo below features a piece in the museum from Morelos, Mexico, representing the creation of man, community, and the universe.
Conclusion:
Magical town Cavillo, with a population of around 60,000, is clean, inviting, and well-organized and worth a weekday visit. It is apparently crowded on weekends and on festival days.
Its streets are flat, its sidewalks comfortable for walking. In a few places there are hills. It sits alongside the Rio Calvillo.
Aging in Place/Aging in Community seems a lot easier in Calvillo than in larger Mexican cities, especially if you are not of high income. There is local social support and love energy.
Wendy Jane Carrel, MA, is an older adult health care advocate, advisor, and care coordinator from California. She has conducted due diligence for senior living and retirement on five continents and is dedicated to supporting families and their elders. She provides informed, attentive, compassionate guidance and curated options for aging in Ecuador, Mexico, and other destinations both domestic and abroad. She is a speaker and published author on subjects related to senior well-being. Wendy’s web site is https://www.WellnessShepherd.com
City streets were abloom with jacaranda and magnolia trees, and sidewalk gardens featured roses, brugmansia, and honeysuckle as the City of West Hollywood, California celebrated Older Adults Month in May 2025.
Aging in Place/Aging in Community resources and services were highlighted, and the city honored a senior who has made a difference in the community.
Since 2016, the Aging in Place/Aging in Community Strategic Plan created to accommodate the anticipated silver tsunami (the worldwide phenomenon of older adults living longer) has been a stand-out initiative. The goal: offer quality-of-life and a sense of control for aging where you live with an extensive array of easy access support services. According to the 2020 census the population of West Hollywood is around 36,000 with older adults 65+ representing 20% of residents (7,200).
A recent West Hollywood Aging in Place success story:
A 92-year-old solo ager was hospitalized after breaking a hip and femur bone. From the time she entered an in-patient rehab she knew she wanted to be at home. Any other place? She felt her life might unravel. The challenge? How to access the only bathroom located upstairs in her one-bedroom apartment. With the good offices of a Jewish Family Services social worker, the woman’s health care advocate who lives almost an hour away, and the non-profit DCRC (Disability Community Resource Center) which serves the disabled, a stairlift was installed so she could continue to enjoy her home of over 50 years. Her health and her spirits improved greatly over a period of months. So greatly that she was able to give a poetry reading from her recently published book at a southern California library the last week of May. She continues to use a walker. The stairlift allows her comfort for healing and self-sufficiency.
Note: In 2022, the City of West Hollywood received the SCAN Foundation Innovation Award for “embracing aging” in one’s home throughout a person’s lifespan.
On May 14 at 2:00 p.m. at the televised Older Adult Advisory Board (OAAB) meeting, Richard (Ritch) Colbert a chaplain at Cedars-Sinai Medical Center and 39+ year counselor for the recovery and LGBTQ communities received the Senior of the Year Service Award with a proclamation presented by Mayor Chelsea Byers and OAAB Vice-Chairman RJ Holguin. Story plus photos at this link: https://wehotimes.com/west-hollywood-honors-richard-colbert-at-20th-annual-older-adults-service-awards/
Older Adult Advisory Board Chairman John Allendorfer deftly guided the televised meeting. During Public Comments Disability Advisory Board member Rick Watts and Human Services Commission member Karen Eyres spoke movingly about current concerns, mainly proposed Medicaid cuts which would harm children, the disabled, and older adults. Medicaid, known as Medi-Cal in California, currently provides essential health care coverage including support for vulnerable older adults for long-term care in nursing homes.
West Hollywood Older Adult Advisory Board members at the 20th Annual Older Adult Health Fair on May 8, 2025 in the photo below. Missing are members Nadia Sutton and A. Lee Walkup.
On May 8 several hundred seniors convened at Plummer Park for the 20th Annual Older Adult Health Fair co-sponsored by Cedars-Sinai Medical Center and Jewish Family Services. Attendees learned about and/or applied for assistance with an array of non-profits:
Access LA transportation services for the disabled
Bez Tezek Free Legal Services
City of West Hollywood Rent Stabilization Department “Know Your Rights” Workshop
One Generation’s program registration for utility assistance and energy conservation
Jewish Family Services social worker support
Jewish Family Services nutrition education and meals at centers around the community
Jewish Family Services exercise and crafts classes, a social engagement monthly meeting, classes in digital education
The California Hearing Center, a family business, offered free hearing assessment tests
Others
Most of these programs/services are free or donation based.
Not present at the fair in 2025 but present last year was Metro.net the LA County bus and rail transportation system which continues to offer West Hollywood older adults $20/month complimentary travel on Metro. Seniors TAP cards are reloaded with the city.
According to Rent Café, approximately 80% of West Hollywood residents are renters. West Hollywood’s Rent Stabilization Department gave a presentation at the fair. Grassroots community organization Coalition for Economic Survival (CES), focused on supporting tenant’s rights since 1973, was also present.
Cedars-Sinai Medical Center offered:
blood pressure readings, blood glucose readings
cholesterol readings, heart rate reports
consultations with an MD
participation for those interested in a Cedars-Sinai free genetic testing research project
The Care Team, active in West Hollywood since the fall of 2023, and at the fair for the first time, offers mobile behavioral health support in partnership with www.sycamores.org. A two-person team cum phone coordinator 24/7, holidays included, mans each shift. They work in tandem with the County Fire Department’s Station 7 & 8 in West Hollywood, and the West Hollywood Sheriff’s station to respond to crisis situations, especially assisting the unhoused and other vulnerable populations “in an atmosphere that empowers”. The team also conducts follow-up care and wellness checks for all who call. The Care Team number is (323)540-6392. Also see www.weho.org/careteam.
Preparing for the West Hollywood 20th Annual Senior Health Fair on May 8 in the photo below are Older Adult Advisory Board Member Pat Dixon (on the left), honored with the 2025 LA County Older Adult Service Award, and Francisco Gomez, Acting Strategic Initiatives Supervisor, City of West Hollywood currently dedicated to the Holloway Interim Housing Program.
A community Aging in Place plan is a privilege. Nationwide surveys reveal 90% of the older adult population prefers to age in place.
West Hollywood is a small, young city of about two square miles sitting on the unceded land of the Gabrieleño Tongva and Gabrieleño Kizh peoples. It is surrounded by the City of Los Angeles. Los Angeles, founded in 1781, has an estimated population of around 3.8 million. Two older adults from Culver City (20-30 minutes away) who attended the health fair last year and this year shared how they wish they could move to West Hollywood. Other older adults who live in Los Angeles county and neighboring Los Angeles have shared similar thoughts with this writer after witnessing and comparing services. (Yes, a smaller population creates a more tenable situation).
In its 40 years as a city, West Hollywood has created a strong bank of social service resources for all citizens, not only seniors. Its Aging in Place/Aging in Community plan won the SCAN Foundation’s Innovation award.
Other age-friendly cities actively developing notable services for health, housing, participation, security, transportation, and more are Rochester, NY; Grand Rapids, MI; Madison, WI; Provo, Utah and others. On the This Old House survey (see resource section below), West Hollywood is listed as number seven out of 10, mostly because the cost of living in California is higher compared to the rest of the cities on the list.
Honoring contributions of older adults each year and addressing their needs in aging officially started by federal government decree in 1963. At that time 17 million older adults were 65 or older, one third lived in poverty, and few programs existed to meet their needs. Today there are approximately 60 million older adults in the U.S., nine million in the State of California.
Disclaimer: The author has lived in West Hollywood, CA since graduate school and has a bias for a community she appreciates living in.
Wendy Jane Carrel, MA, is an older adult health care advocate, advisor, and care coordinator from California. She has conducted due diligence for senior living and retirement on five continents and is passionate about supporting families and their elders. She provides informed, attentive, compassionate guidance and curated options for aging in Ecuador, Mexico, and other destinations both domestic and abroad. She is a speaker and published author on subjects related to senior well-being. Wendy’s web site is https://www.WellnessShepherd.com
Resources:
https://acl.gov/oam/history# Administration for Community Living website (formerly Administration on Aging website)
If you live in Mexico or Latin America, have you created a plan for what to do in case of an accident, natural disaster, or healthcare emergency?
Who is going to show up for you?! What if you are no longer able to speak and make decisions for yourself?
If you wish to save your family and other loved ones considerable grief and time, it is important to understand what is involved when a foreigner becomes ill or dies in Mexico or other Latin American nation.
Last month I had the pleasure of joining patient advocate and educator colleague Deborah Bickel of Be Well San Miguel to share with expats why it is wise to create a Mexican declaracion jurada (living will) and/or voluntad anticipada (advance healthcare directive). The voluntad anticipada is incorporated into the declaracion jurada in many sates. My role in the meeting was to give an overview of palliative care and hospice and how to find end-of-life support in Mexico.
We have each invested 14 years or more sharing with expats (Deborah in Mexico, Guatemala, and Nicaragua – me in Mexico and Ecuador) why planning is important no matter your age but especially if you are 55+.
Short list of reasons:
Mexican law is civil law
British, Canadian, and U.S. law is common law.
There are major differences.
If you arrive with an Advance Healthcare Directive or Five Wishes or other document legal in your native country, it will not be legal in Latin America unless you get lucky. In Mexico, you must create a declaracion jurada and/or voluntad anticipada if you want your wishes to be honored. Some attorneys and notaries will incorporate your home country wishes for you. These documents must be created BEFORE any accident, illness, or demise. As of this date only 14 of Mexico’s 32 states offer a voluntad anticipada. The purpose of the voluntad, sometimes referred to as a directriz, is to avoid legal, medical, and bioethical problems that could complicate the situation for you the patient or your family.
Mexico is a country with predominantly Catholic traditions. These traditions influence choices. If you are Catholic, the system may seem familiar, such as burial over cremation. If you had chosen to live in Buddhist or Hindu Asia, cremation would be a relatively easy matter involving fewer steps as cremation is common practice. Or, you could have opted for a Tibetan sky burial. If you wish to be cremated, you will need a notarized document stating this wish.
Latin Americans have large family systems. If something happens to you as a Latin American, a family member will show up and know what to do. Most expats live in Latin America alone or as a couple, sometimes with children.
The Mexican culture, language, and way of thinking are unique. Most of all, procedures may be unfamiliarand complex. Attitudes and response to accidents, illness, and death are different.
Non-Spanish speaking expats often need bilingual advocates to negotiate the system. At least three people are recommended to advocate for your wishes, and/or serve as your healthcare proxies. If one is not available, perhaps another will be.
April 16 is National Healthcare Decisions Day in the U.S. If you do not yet have a plan, every day is a good day to work on one no matter where you are.
Aileen Gerhardt, a fellow patient advocate and educator in Boston writes “decide, document, designate, and discuss!!” Good advice.
Wendy Jane Carrel, MA, is a Spanish-speaking senior care advocate from California. She has travelled Mexico for several years researching health systems, senior care, and end-of-life care to connect Americans, Canadians, and Europeans with healing options for loved ones. She is a compassionate companion and palliative care liaison, legacy writer, co-founder of Café Mortality Ajijic/now Death Café Ajijic and founding member/speaker of the Beautiful Dying Expo (USA). She is a trauma-informed, gentle End-of-Life Doula (National End-of-Life Doula Alliance proficient), and a speaker and published author on subjects related to senior well-being. Wendy’s web site is https://www.WellnessShepherd.com
The holiday season for many in the northern hemisphere is sometimes fraught with sadness, sorrow, and a sense of loss. Thankfully, there is an invitation for comfort and a unique panacea of sorts… a Grief Choir.
What is a Grief Choir and how did I end up attending one?
Elizabeth Gill Lui, the thoughtful leader of Death Café at the Los Angeles Philosophical Research Society, has a mailing list. I am thankfully on it. Her interests and friendships are deep and wide from experiences as a fine arts photographer, author, educator, end-of-life doula, and more.
I read about the gathering and felt compelled to attend.
So, on December 22, at the time of the solstice (shortest and darkest day of the year, but also the birth of light), I found my way to the First Congregational Church of Los Angeles to listen to a choir. I was curious.
Here is what happened:
I arrived late, by minutes.
About 30 folks were gathered quietly on chairs in a circle.
The Resonance Collective hosts, Artistic Director Fahad Siadat and clinical psychotherapist Cynthia Siadat smiled in my direction and welcomed me warmly. Someone added a chair so I could join the circle. Lovely.
The leaders shared…they created the concept of Grief Choir out of “a desire to hold space outside a particular religious context during times of loss.” The gathering was intended as a ritual “to sit with the darkness of grief and the growing light of the community with whom it is shared.” A special event, free, to sing and heal. No experience required.
Cynthia passed around a basket with pens and white cards. She asked attendees to write three words for why they came. The cards were collected in the basket and passed around again. This time each of us picked a card from the basket. Then we read aloud from the card we picked. Many reasons were remembrances – names of persons (or pets) who had passed. Do not know for certain as do not know who wrote the names or why. Touching to listen to, especially since none of us knew each other, and a way to feel connected to the community of 30.
Below is a photo of the First Congregational Church of Los Angeles meeting room. For reasons of privacy, no photos of the gathering on the other side of the bridge table.
Fahad then introduced the East Indian wooden shruti box, akin to a harmonium, sitting on his lap.
If interested, you may read about the shruti box here:
The box has bellows. Fahad slowly opened and closed the box like an accordion. There was no melody, but a drone sound with each movement. And then Fahad would hum and guide a sound meditation. The group was invited to respond and hum with him. A call to grief if you will. The sounds defied description.
This was quite a surprise for me as I thought I had attended to listen to a choir. As it was then apparent, the choir consisted of all who attended, me included.
The humming at times took on the sound of gentle, tender, almost-wailing. Difficult to describe, intangible, something one must experience. Perhaps a bit of the ululations (zagrouta in Arabic), bouncing from lament to joy but not exactly that. Most of all, a feeling of support from others in the circle. Eyes were closed or open. Fahad and Cynthia had created a safe space. Mellow feelings at the end of the hour.
Fahad (imagine a modern-day Sufi or Rumi) has been described by the LA Times as a “fanciful and downright utopian artist and thinker”. His bio states he “explores sound as spiritual practice, creating interdisciplinary pieces as a vehicle for unveiling the mystery of our interconnected world.” An apt description.
I am pleased to have attended. Unique and memorable. For those who are in Los Angeles and interested, the next Grief Choir is scheduled for the Summer Solstice somewhere around June 20, 2025. The announcement will be made on the Resonance Collective website.
For information about the Resonance Collective and Fahad Siadat see:
Wendy Jane Carrel, MA, is a Spanish-speaking senior care advocate from California. She has travelled Mexico (and Latin America) for several years researching health systems, senior care, and end-of-life care to connect Americans, Canadians, and Europeans with healing options for loved ones. She is a compassionate companion and palliative care liaison, legacy writer, co-founder of Café Mortality Ajijic/now Death Café Ajijic and founding member/speaker of the Beautiful Dying Expo (USA). She is a trauma-informed, gentle End-of-Life Doula (National End-of-Life Doula Alliance proficient), a speaker and published author on subjects related to senior well-being, and serves on the City of West Hollywood’s Older Adult Advisory Board. Wendy’s web site is https://www.WellnessShepherd.com



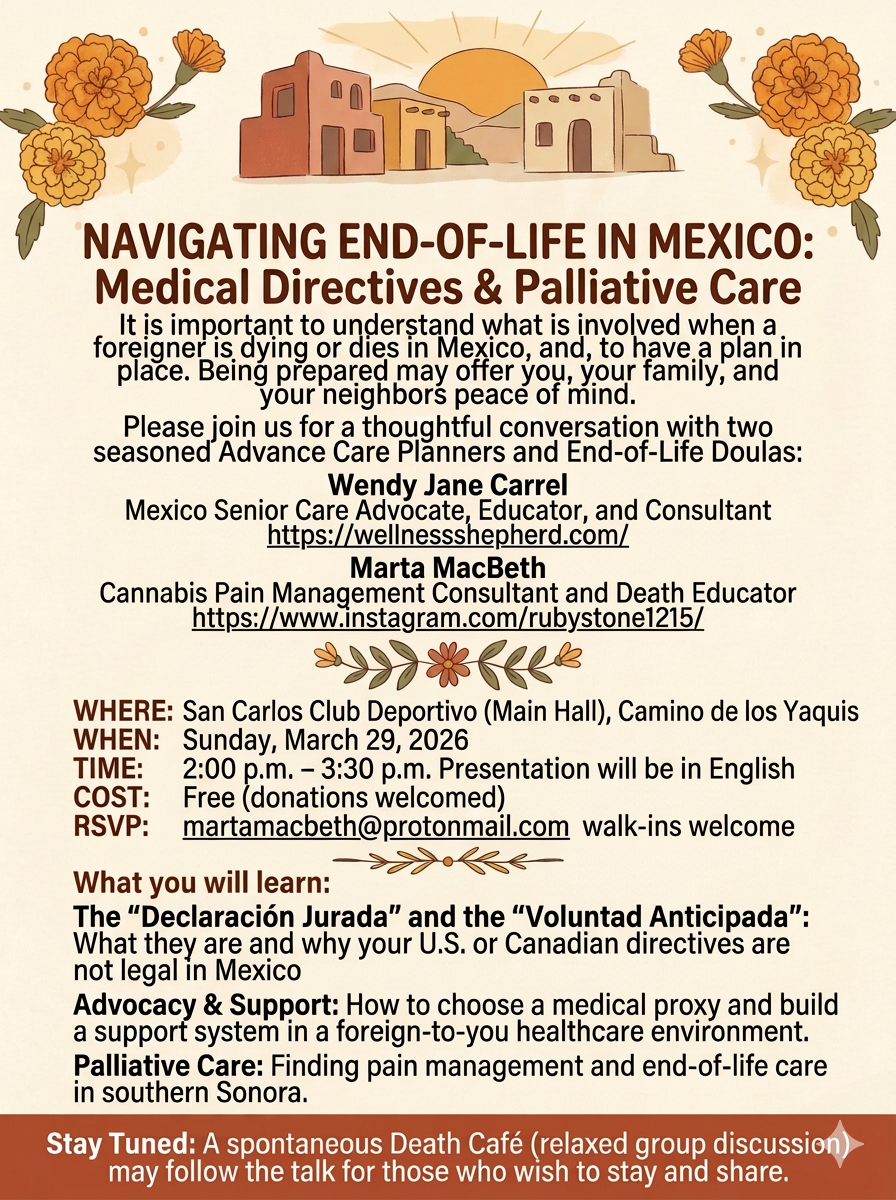

















































{kind=link}